This article was originally published on The liberty Beacon. You can read the original article HERE
ER Editor: Readers of this site know that we have published criticisms of Dr. Pierre Kory that we stand by. However, that doesn’t mean that Kory cannot write a decent, informative piece about cognitive problems among his heavily-vaccinated colleagues. Further, those colleagues extend into a great many countries, including European ones. It isn’t just an American problem, although we are more likely to get information about this topic from there.
What he calls ‘Long Covid’ below (medical symptoms following Covid, not the vaccine) we prefer to think of as illness from a bioweapon.
********
Are Medical Errors On the Rise Due To Cognitive Impacts Of The mRNA Vaccine?
In a three day span, I was told by four different patients of errors made by both physicians and nurses that harmed them, ranging from the catastrophic to the concerning.
Pierre Kory, MD, MPA
As the title of this post reflects, I recently developed a growing concern that health care providers are “not as sharp” as they used to be and, as you will learn from the cases I will present below, that may be putting it mildly.
Why would I hypothesize about a sudden deterioration in the cognitive and technical abilities of health care providers? Couple of reasons;
The most mRNA vaccinated sub-population in the United States are almost certainly our health care providers.They make up the entire class of employees mandated by the Centers for Medicare and Medicaid Services (CMS), the agency that governs the two federal/state health insurance plans for the elderly and poor. Recall that 25 states fought back against CMS by issuing injunctions against the mandate until the Supreme Court granted CMS the authority to do so. Which meant that all CMS facility employees (every hospital, nursing home, and home health agency employee in the country) had to get the mRNA vaccine otherwise they would not be eligible for reimbursement for their services from those entities. That does not make for a valuable employee.
The mRNA “vaccine,” like Covid itself, causes immense amounts of cognitive dysfunction, i.e. “brain fog” and worse. In my Leading Edge Clinic specialty practice where we treat Long Covid/Long Vax (70% are Long Vax) of the almost 1500 chronically ill patients we have encountered, the vast majority report new-onset cognitive dysfunction.
The real tragedy is that the mandate from CMS specified that “accommodations” (i.e. exemptions) should be offered by the involved health care facilities; however, as we well know, in the vast majority of facilities, exemptions were nearly impossible to obtain. Numerous lawsuits are ongoing to address the horrific negative consequences of the mass firings that resulted. The bright side is that I am hearing from my Covid litigation experts that these cases are now being regularly won.
However, the behavior of the many corporate health systems around the country effectively “weeded out” all unvaccinated employees. Although a number of centers apparently now welcome back their former unvaccinated employees, it appears that not many as hoped wanted to return to a former employer that treated them that way. Thus, I maintain that the vast majority of those currently working in the system are vaccinated, and heavily vaccinated at that.
So, if they are so heavily vaccinated, what is the probability that they are suffering cognitive issues? Well, from my recent (surprisingly popular) post about the goings on at Ohio State Medical Center, apparently numerous docs were retiring or going out on disability due to “neurological issues.”
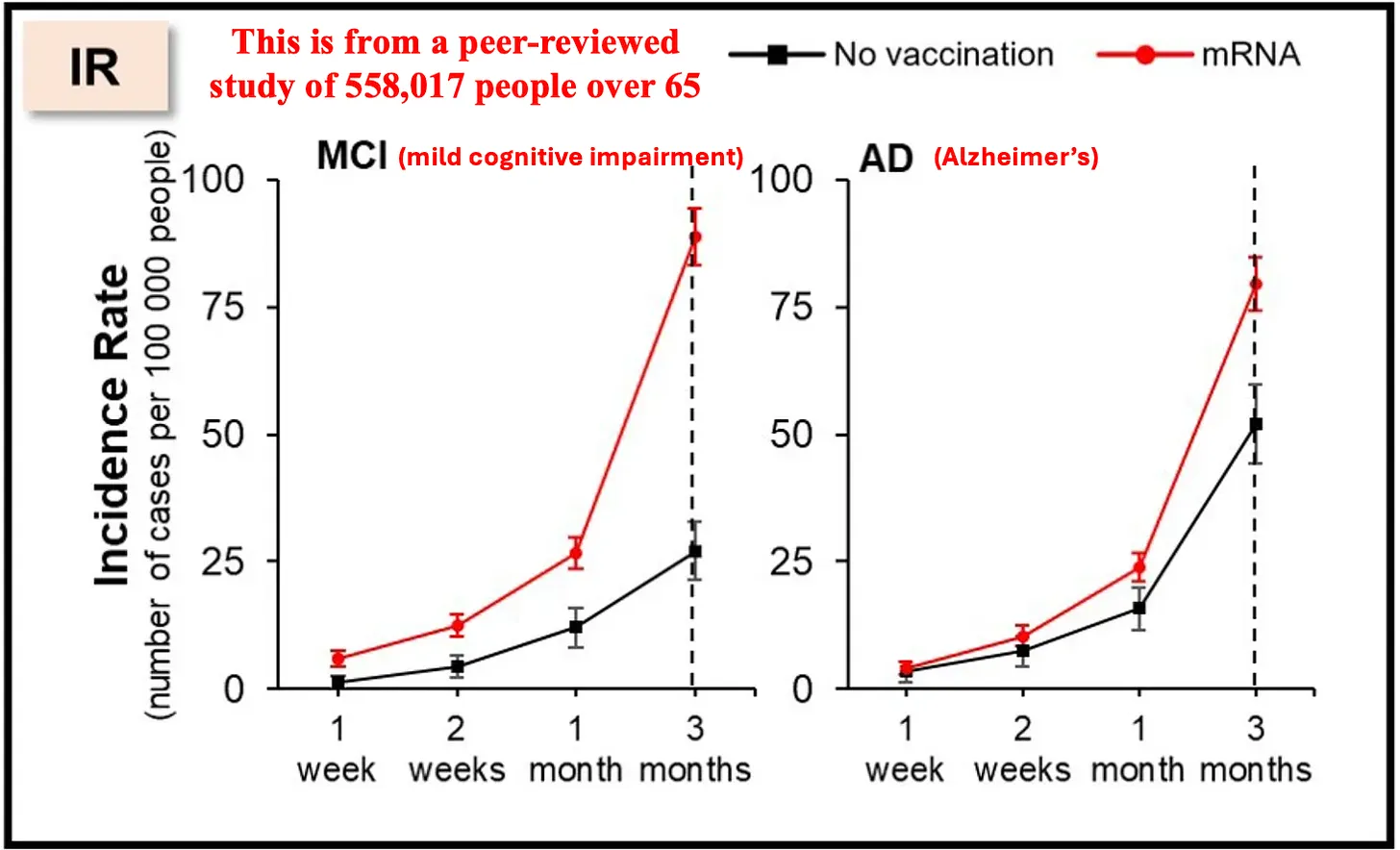
The “anecdotes” I cited in that post are further supported by two recent papers out of South Korea which found shocking negative impacts on cognitive abilities in those who underwent mRNA vaccination. A Midwestern Doctor did an excellent job in not only analyzing that paper but also putting the Korean studies into the context of what we already know about the cognitive impacts of the mRNA platform. I am going to bullet some of the numerous data points AMD cited, beginning with the South Korea studies which analyzed a large database of the inhabitants of Seoul where vaccination status was accurately recorded. It’s not good:
One of their papers published in Nature (one of the top medical journals) found a 68% increase in depression, a 44% increase in anxiety, dissociative, stress-related, and somatoform disorders, a 93.4% increase in sleep disorders, a 77% decrease in schizophrenia, and a 32.8% decrease in bipolar disorder.
Another of their analyses was published by the senior author, again in a mainstream journal. It analyzed individuals over 65 and found COVID vaccination increased the risk of mild cognitive impairment 138% and the risk of Alzheimer’s by 23%, and a smaller increase in vascular dementia and Parkinson’s disease the authors did not deem to be significant.
In line with the above, I will include a couple of “anecdotes” written as subscriber comments to AMD’s article which I found unsurprising and in keeping with my own professional experience and the data above:
Thank you for confirming what many of us have known for years. Within a few months of the jab, my mother developed severe cognitive issues. I personally labeled it ‘sudden onset dementia.’ The doctors have not diagnosed her issues as dementia but I worked on an Alzheimer’s/Dementia unit years ago and the patients exhibited similar symptoms.
And another one:
Can confirm cognitive impairment is real. Nearly lost my job because my short term memory was severely impaired. Could not remember the 6 digit code generated by a crypto card used for signing on to computer systems. I had to enter 1 number, look down at the card again, enter 1 number, look again. This was just one of the manifestations. More complex equations, calculations and datasets were jumbled strings of nonsense. Finally got the info to go see a FLCCC affiliated physician and they started me on the very long road to some form of normalcy and productivity. I still have episodes of brain fog and multi-hour stretches where I’m unable to concentrate on complex topics, but the productive hours greatly outnumber those in deficit.
I myself had a close colleague who, in 2021, had to stop rounding in the ICU for several months after the mRNA vaccine because they couldn’t remember critical details. Another colleague, Dr. Robert Jackson in Missouri, is a truly brilliant rheumatologist who has helped me develop and refine my therapeutic approaches in my Long Covid/Long Vax practice. He relayed to me that when he got Covid in late 2020, he developed “brain fog” that was somewhat manageable, but then after his vaccine in Feb. 2021, the cognitive deficits were greatly amplified (think spike in brain). The symptoms became so pronounced that he thought he was going to have to retire. He told me he would stare off into space, could not remember critical details, could not process or organize tasks etc. Luckily he found therapies which reversed this issue and he did not have to retire.
FURTHER EVIDENCE OF COGNITIVE HARMS
Lets go through some more of the evidence of cognitive harm, some of which I compiled myself, but I also liberally borrowed from AMD’s comprehensive review titled, “We Now Have Proof The COVID Vaccines Damage Cognition.”
I will bullet some of the major data sources they found:
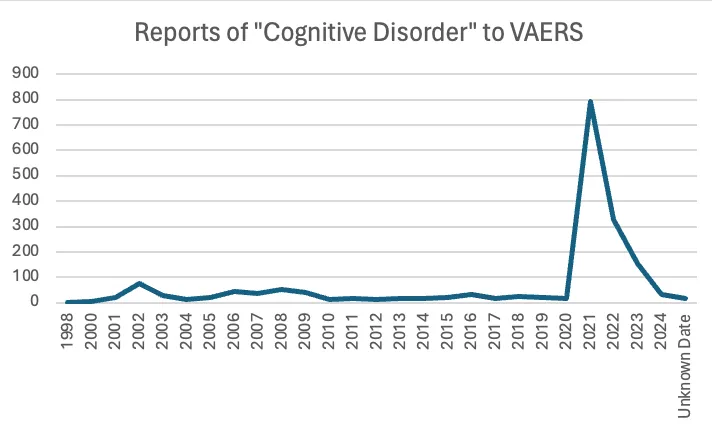
VAERS detected a massive spike in cognitive issues being reported to it after the COVID vaccines hit the market.
I own a small business and deal with many people and other small businesses. Most provided reliable service, would remember appointments, followed up on issues, and so on. I noticed that lately, some people have become less capable cognitively. They forget essential appointments, cannot concentrate, make crazy-stupid mistakes, and so on.
Igor’s anecdote above was also supported by one of my best and oldest friends who is the mayor of a village of over 3,000 inhabitants. He reported to me that he finds he has to do a lot more tasks at town hall because things he used to be able to delegate kept not getting done or got done incorrectly.
Igor Chudov also identified another dataset from the Netherlands which further corroborated a massive cognitive decline:
In the first quarter of 2023, there was a 24% increase in GP [general practitioner] visits related to memory and concentration problems among adults (age 25 years and older) compared to the same period in 2020. This is evidenced by the latest quarterly research update from the GOR Network.
More specifically they found: •No increase was observed in adults under 25 years old. •A 31% increase was observed in those 24-44 years old. •A 40% increase was observed in those 45-74 years old. •A 18% increase was observed in those over 75 years old.
Now, although I have not yet presented the anecdotes of the medical errors reported to me yet, I initially questioned whether they were “Vaxxidents.” One of the reasons I used the word “Vaxxident” is that I have been aware for a while now that motor vehicle accidents greatly increased during the pandemic. Since they started to increase in 2020 before the jabs, obviously that suggests that Long Covid may be a significant contributor, but the greater increases in 2021 suggest the jabs may have compounded the issue, almost like the case of Dr. Robert Jackson above:.
The above chart and the comments below are taken from the Substack of the brilliant actuary Mary Pat Campbell from her posts on the rise in motor vehicle accidents. Note that she hypothesizes that the rise was largely due to less people on roads and thus faster speeds, but, as you can tell, my hypothesis is a bit different. Anyway, she wrote:
The low for the period above occurred in February 2010, when there was only an average of 77.9 motor vehicle accident deaths per day.
Before that, the local high had been in July 2007, at a high of 141.6 deaths/day. The most recent high occurred in October 2022, at 144.6 deaths/day. Interesting it took 15 years to get back to that level… and that’s not a good thing.
Then I picked out January 2022 — it was a low point for 2022, and January tends to be a low point for most years.
But I picked it out specifically so you could compare it against the rates in 2018 and 2019. That low in 2022 is only a few percentage points below the high from the pre-pandemic rates.
Also, per Brave Browser AI: “Record high in 2022: Fatal car crashes reached a record high in early 2022, with road safety experts attributing this to pandemic-fueled risky driving behaviors such as fewer seat belts, more speeding, and impaired driving.”
If you look at the full historical data on traffic fatalities in Wikipedia, one data point jumped out at me, which is that in 2021 there was an 11.1% increase in per capita traffic fatalities compared to 2020. Not since 1945 has there been a double digit percent increase in this metric from one year to the next.
AMD’s post even included a quote from me, which I will include (thus I am citing someone who is citing myself – weird 🙂
In my practice of treating vaccine injuries, one of the three most common symptoms I see is brain fog. So many of my patients had been in the prime of their lives, can now barely function, have significant cognitive impairment and need a lot of help from our nurses to carry out their treatment plans. I never imagined I would see any of this in people far younger than me and instead I see it every day. I bear witness to an immense amount of suffering on a daily basis that is hard to put into words.
PATIENT REPORTS OF PROVIDER ERRORS
Now, to the point of this post, I will present a few cases of poor medical care which I think may have resulted from the adverse impacts of the mRNA vaccines. Let me state from the outset that I have no direct evidence that in these cases the physicians were vaccinated or that they had cognitive deficits from the vaccine, and I also must recognize that Long Covid (ER: bioweapon?) can cause cognitive issues/brain fog as well. However, like the three Uruguayan soccer players who collapsed within a week of each other (presented in my last post), the four cases below came to my attention in a three day span.
If I am being unnecessarily alarmist or insufficiently prudent by raising concern over the cognitive health of doctors in the U.S medical system, forgive me. I figured this Substack is a safe place “to be real” with my theorizing so here goes.
Case 1 – I saw a young woman with metastatic osteosarcoma whose parents consulted me for complementary cancer care. Initially her tumor was isolated to her leg and she needed it resected. Her family consulted what they described as a “highly experienced surgeon of over 30 years regarded by many to be the most skilled in the area.” However, after leaving the operating room (OR), tragedy ensued when she had to be brought back to the OR on the same day due to excruciating and unrelenting pain. The 2nd operation required numerous other specialty surgeons (vascular and nerve) to be brought in to assist in repairing what was essentially (not literally) described in the record as consistent with a “botched” surgery. Apparently, the surgeon failed to reconnect major arteries and nerves. This led to her undergoing a total of 6 surgeries in a 35 day hospital stay, and although she was discharged with two legs, the botched leg eventually proved non-functional and was subsequently amputated 9 months later. Note she is a teenager. Vaxxident?
Case 2 – A day later I saw a patient with a chronic fibrosing lung disease, likely autoimmune in nature and who has been on a strong immunosuppressant for over a year. The good thing is that when reviewing her records, and in particular, her pulmonary function testing over the past year (four of them in total), numerous indices of lung function showed steady, significant improvements every 3-4 months and clinically she was regaining exertional tolerance etc. However, she was upset because she told me that the pulmonologist who had been treating her over the past year had been repeatedly telling her that her disease was severe and getting worse, until finally, in the visit the day before she saw me, he realized that her lungs had actually gotten better and told her so. She got upset with him for causing her so much anxiety over the past year that she fired him. Note he did not apologize and instead reminded her of his credentials and experience. My take is that when looking at the chart of her lung function indices, instead of looking at them chronologically from left to right as they were arranged (they are not always done this way), he had been looking right to left and thus misdiagnosed her as worsening. Vaxident?
Case 3 – A day after the above two cases, a colleague sent me an article about the case of a surgeon who removed someone’s liver instead of the spleen (the planned surgery). Note the spleen is on the way left side of the abdomen and the liver is on the right, and they look little like each other. Plus removing livers is not a thing (unless you are transplanting). The same surgeon, in 2023, also removed parts of someone’s pancreas instead of doing the intended surgery of removing the adrenal gland. Vaxidents?
Case 4 – the wife of a patient told me in passing about her 88 year old mother’s recent ER visit for atrial fibrillation where she needed electrical cardioversion. The patient told me how upsetting it was being there because no-one was communicating with her about how her mother was doing with the cardioversion. She finally was able to engage with a nurse and asked her about how her mother’s cardiac rhythm was doing. The nurse looked at the cardiac monitor station and told my patient that her mother’s rate and rhythm were “just fine.” When my patient pointed out that, to her untrained eye, the rate and rhythm appeared quite abnormal on the monitor that was in her mother’s actual room. The nurse looked again at the monitors and said “sorry, let me get the doctor to come talk to you.” Vaxxident?
PHYSICIAN ERROR RATES SINCE THE PANDEMIC
So, given the data above supports a hypothesis that physicians may be committing more errors than in the past, or at least have cognitive dysfunction which would lead to that, does available data support this hypothesis, i.e. is there data showing increases in physician errors, malpractice lawsuits, or complaints against physicians since the roll-out of the jab campaign?
One problem with proving that using existing data is that as I started to research, I quickly discovered something that researchers in the field have long recognized that papers and databases on medical errors have varied rates due to variabilities in reporting, geography, general health disparities etc. I found it difficult to find one source that presented rates year by year. The best paper that I could find which studied medical errors was done by Hopkins and published in JAMA in 2019 here.
It was a study of a representative sample of hospitals consisting of patients who went to ICU and/or died in hospital:
23% experienced a diagnostic error while hospitalized (wow).
Errors were judged to have contributed to temporary harm, permanent harm, or death in 436 patients (17.8%)
Among the 1863 patients who died, diagnostic error was judged to have contributed to death in 6.6%
Again, that was from 2019 and I could find no more recent analysis to compare to. So I then looked at the National Provider Data Bank, which logs malpractice claims against physicians. Although there were drops in 2020 and 2021, note that these claims are recorded only when paid out, not when filed, so we will not know for a couple of years at least whether malpractice suits have gone up. The drops in claims during 2020 and 2021 likely reflect the impacts of Covid measures on the courts.
SENTINEL EVENTS
What I did find was disturbing trend of data regarding “sentinel events” in hospitals. First, lets go over the definition of a sentinel event:
A “sentinel event” is an unexpected occurrence in a healthcare setting that results in:
Death
Permanent harm (e.g., loss of limb or function)
Severe temporary harm (e.g., significant disability or disfigurement)
These events are not related to the natural course of the patient’s illness and are often caused by major mistakes or negligence on the part of healthcare providers. Sentinel events are closely investigated by healthcare regulatory authorities to identify root causes and implement corrective actions to prevent similar incidents from occurring in the future.
There are 58 total types of sentinel events, with the most prevalent being:
Falls (48%)
Wrong site surgery (8%)
Unintended retention of foreign object (8%)
Assault/rape/sexual assault/homicide (8%)
Delay in treatment (6%)
Suicide (5%)
Check out the below data chart from the Joint Commissions 2023 review of sentinel events which shows a steep rise in sentinel events concurrent with the roll out of the mRNA platform (obviously other factors likely contribute but the temporal association should give serious pause):
Now, before I go through the major sentinel events, I found this sentence in the beginning of the report:
“As the reporting of most sentinel events to The Joint Commission is voluntary, no conclusions should be drawn about the actual relative frequency of events or trends in events over time.
That sentence reminds me of the U.S. Society of Actuaries report where they also cautioned against making any conclusions regarding the temporal relationship of the massive rise in life insurance claims with the rollout of the mRNA platform and/or mandates as I discussed in a previous post here. The Joint Commission’s statement above is as absurd when you look at the chart – sentinel event reports are remarkably stable from 2013-2020 and then shoot up dramatically starting only in 2021 (and remain high).
So, what sentinel events drove this rapid rise?
Answer: FALLS!
Contrary to my original hypothesis, there really isn’t much of a signal supporting an increase in physician errors in the above data. Delay in treatment can be explained by Covid surges and staffing issues (from mandates), but, at the risk of cherry picking data, I highlighted “Wrong Site Surgery” as being problematic in 2021 even though it was less than 2019. The reason I highlighted this is that a “wrong site surgery” is truly supposed to be a “never event” and many systems and processes have been put into place to avoid this happening over the past decade. Thus I felt the sudden rise in 2021 concerning. It also rose again by a large amount in 2023. But, since both were lower than in 2019, I can’t make a strong argument with this data except to say these should be consistently decreasing year by year but they are not.
But the real issue to discuss is… falls. The average number of falls in 2019 and 2020 nearly tripled in 2021 and then became a quadruple of the pre-mRNA campaign rate in 2022 and 2023. Admittedly this can be from increasing cognitive impairment of patients but also likely represents less monitoring/care/training of nurses (issues which were discussed in my previous post here). But the real shock is what the Joint Commission wrote in their report:
Conclusion: Reported sentinel events remained consistent with previous reporting patterns. Consistent with previous years, patient falls were the leading event type reviewed (48%).
I found the above statement overtly misleading in that although yes, the highest percentage of sentinel events were falls in “previous years,” if you look below to see what percent were falls prior to the jab campaign – only 18-21%. Now they are almost 50% and the absolute number of falls reported has skyrocketed.
I think the Joint Commission headline and conclusion should have been “Alarming Increase in Patient Falls In U.S Hospitals (since the mRNA campaign)” or, to be less inflammatory, “since 2021”. I cannot emphasize how serious this change is. First off, know that historically 3% of all hospital patients fall and 30% of those patients suffer injury.
From the Joint Commission Report:
26 deaths from falling in a hospital? 56 falls resulted in permanent harm and 538 resulted in severe harm?
Why is there not a big national push to prevent falls in hospitals if they have suddenly risen at such an acute and unprecedented rate? This metric, in my mind, is literally screaming that hospitals are now much more dangerous places given they are unable to prevent falls among the patients they take care of. Again from the report:
Consistent with 2022, patient falls while ambulating was the leading mechanism for falling followed by falling from bed and falling while toileting. Reported contributors to falls included policies not being followed (e.g., fall risk assessment), lack of competency to recognize abnormal clinical signs or signals, inadequate staff-to-staff communication during handoffs or transitions of care, and lack of shared understanding or mental model regarding plan of care.
I found it interesting that they highlighted only causes related to poor monitoring, communication, and care by staff when there are numerous other contributors that are more patient driven, like:
unfamiliar settings
medicines that cause dizziness and confusion.
illness, tests and treatments that make you weak and unsteady on your feet.
lack of activity/weakness
I disagree with the Joint Commission’s position that you cannot compare rates over time because reporting is “voluntary.” I would agree with them if they could provide either data or a rationale that could explain why “voluntary reporting” of falls suddenly skyrocketed in 2021 and that increase was maintained in 2022 and 2023. Was there a big public push to health care institutions and employees to report more sentinel events or falls specifically? They certainly did not provide evidence of that and further, such dramatic increases did not happen for any other sentinel event type.
Unlike JCAHO, I would argue that this sudden and massive drop in the quality of care hospitals provide is a major issue that should be addressed in a systematic, public manner. Is a Congressional hearing warranted?
Even if the data were not consistent with an increase in falls but rather an increase in reporting, wouldn’t you want to confirm that or rule it out before simply ignoring the signal that falls are a new and major issue in hospitals? My cynicism and lack of trust in how our “authorities” confront inconvenient data knows no bounds at this point and this is yet another example.
During my “system” career, I saw that nurses were heavily focused on preventing falls, by doing risk assessments and assigning 1:1 observation of patients with paid “companions” for those at high risk of falls etc. Patient falls were a big deal for everyone involved, chief among them obviously was the patient injured or who often had to get a CT scan of the head or X-rays of the hips to rule out serious injury. But falls are major issue for nurses. A patient fall is like the worst thing for hospital quality data and for the record of the nurse in charge of the patient, yet we suddenly started losing the war against patient falls? And badly too.
Ultimately, although I could not find robust data supporting an increase in overall physician errors or complaints (yet?), the data on falls in hospitals is truly alarming. I believe is reflects an alarming drop in the quality of hospital care due to the training and competence of nurses and/or their cognitive abilities in the wake of the mRNA campaign. To think that the Joint Commission is not raising an alarm because these data are “voluntary” is both inappropriate and nonsensical. Why wouldn’t you start investigating the issue using the hypothesis that reporting of falls has increased because falls have increased and not because quality reporters are suddenly and inexplicably more willing to report falls? Clown world again.
Either way, if I had a loved one in the hospital at risk of a fall, I would make sure a family member or friend was with them at all times or as much as possible.
I just want to say thanks to all my subscribers, especially the paid ones! Your support is greatly appreciated as it allows me to devote what is often large amounts of time in researching and writing my posts, so again, thanks. – Pierre
The Liberty Beacon Project is now expanding at a near exponential rate, and for this we are grateful and excited! But we must also be practical. For 7 years we have not asked for any donations, and have built this project with our own funds as we grew. We are now experiencing ever increasing growing pains due to the large number of websites and projects we represent. So we have just installed donation buttons on our websites and ask that you consider this when you visit them. Nothing is too small. We thank you for all your support and your considerations … (TLB)
••••
Comment Policy: As a privately owned web site, we reserve the right to remove comments that contain spam, advertising, vulgarity, threats of violence, racism, or personal/abusive attacks on other users. This also applies to trolling, the use of more than one alias, or just intentional mischief. Enforcement of this policy is at the discretion of this websites administrators. Repeat offenders may be blocked or permanently banned without prior warning.
••••
Disclaimer: TLB websites contain copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available to our readers under the provisions of “fair use” in an effort to advance a better understanding of political, health, economic and social issues. The material on this site is distributed without profit to those who have expressed a prior interest in receiving it for research and educational purposes. If you wish to use copyrighted material for purposes other than “fair use” you must request permission from the copyright owner.
••••
Disclaimer: The information and opinions shared are for informational purposes only including, but not limited to, text, graphics, images and other material are not intended as medical advice or instruction. Nothing mentioned is intended to be a substitute for professional medical advice, diagnosis or treatment.
This article was originally published by The liberty Beacon. We only curate news from sources that align with the core values of our intended conservative audience. If you like the news you read here we encourage you to utilize the original sources for even more great news and opinions you can trust!
Postal ServiceYubNub Digital Media361 Patricia Drive New Smyrna Beach, FL 32168
E-mail admin@yubnub.digital
Follow Us
About
YubNub! It Means FREEDOM! The Freedom To Experience Your Daily News Intake Without All The Liberal Dribble And Leftist Lunacy!.
Our mission is to provide a healthy and uncensored news environment for conservative audiences that appreciate real, unfiltered news reporting. Our admin team has handpicked only the most reputable and reliable conservative sources that align with our core values.























Comments